Classification of leg shape (Artemyev A.A., 2001)
- Ideal legs
- True O-shaped curvature (varus deformity)
- False curvature
- True X-shaped curvature (valgus deformity)
O-shaped curvature (varus deformity) is the most common reason for cosmetic orthopaedic leg correction — about 15–20 times more frequent than X-shaped curvature.
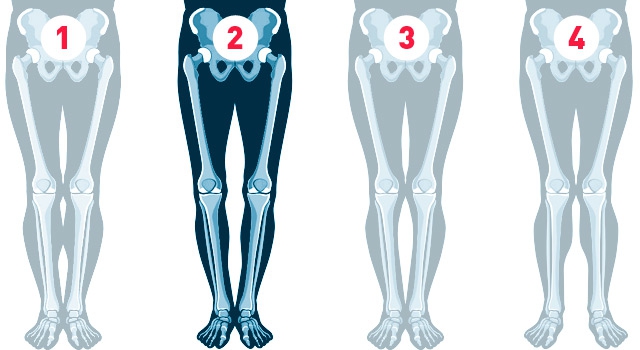
Using the classification it is easy to determine your own leg shape and decide whether anything needs to be changed.
It is very important that timely correction of leg deformity not only produces an excellent aesthetic result, but also prevents the development of knee-joint disease in adulthood and old age. Incorrect load distribution in varus deformity leads to uneven, premature "wear" of the knee joints.
Therefore, timely correction of leg curvature is a way to prevent knee-joint arthrosis.
You can be sure that we will achieve ideal legs in virtually any case. The only question is how long the process will take. We offer three methods for correcting varus deformity of the legs:
Express methods use intramedullary nail fixation, which significantly shortens rehabilitation — active rehabilitation can begin as early as 19 days after surgery.
If you believe you have false curvature — see the dedicated section.
The general principle of leg-shape correction is bone osteotomy in the zone of deformity and consolidation in the correct position.
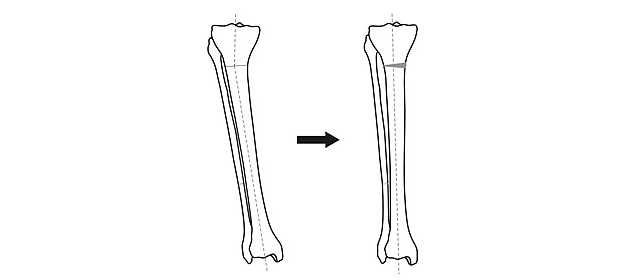
An osteotomy does not require a large skin incision — a small (5 mm) puncture and a single suture are enough. With an aesthetically favourable distribution of soft tissues, an excellent result can be achieved without fully transecting the bone, simply by partially breaking it from one side. This shortens the treatment by 5–15%.
After the bone is cut (osteotomy), the axis of the limb must be brought into the correct position and fixed there until consolidation.
X-shaped deformity is corrected in the same way — only the direction of bone-fragment displacement is opposite.
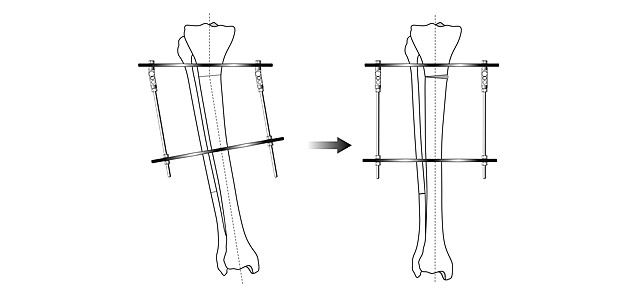
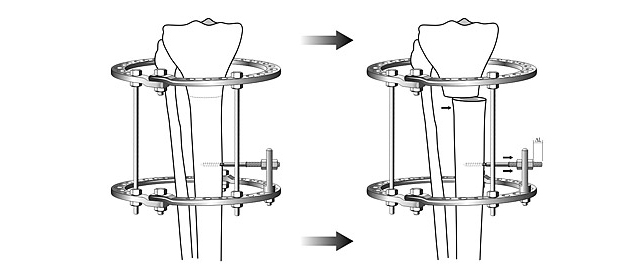
The ideal device for bringing the limb axis into the correct position and fixing it is the Ilizarov apparatus. The greatest experience with the Ilizarov apparatus has been accumulated in Russia. We have been using this method for aesthetic leg correction since 1996, performing more than 1,500 corrections and lengthenings of the thigh and lower leg in a wide variety of conditions.
The Ilizarov apparatus allows you to:
Simplified open-frame constructions have limited capabilities. Meanwhile the Ilizarov apparatus easily fits under trousers and weighs only 900 grams.
Angular correction is the simplest way to correct leg shape. Using the Ilizarov apparatus, any curvature — regardless of type and severity — can be corrected at the patient's request.

An essential condition for an excellent result with angular correction alone is an aesthetically favourable distribution of soft tissues — when the calf muscles lie along the inner surface of the lower legs. The reason is the way the head of the gastrocnemius attaches, not that the muscles are "underdeveloped". Physical exercise will not lead to success here.
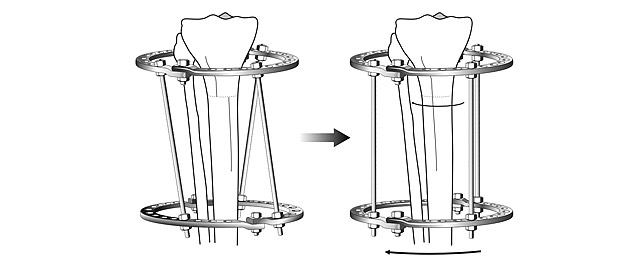
When correcting varus deformity, medialization can be performed simultaneously, significantly improving the aesthetic result.
Medialization is the inward displacement of the peripheral (lower) fragment of the tibia after osteotomy. In modern wire-rod devices this procedure is performed at the patient's request — practically painlessly and gradually — by turning the rods during curvature correction.

At the patients' request, angular correction is supplemented by medialization in almost 60% of cases and significantly enhances the aesthetic effect.
Rotational displacement results from the limb being twisted around its longitudinal axis.

This deformity occurs in 2–3% of cases and can be unilateral (asymmetric) or bilateral. Rotation correction is performed in pronounced cases or in case of asymmetry between the two legs.

A prominent fibular head combined with varus deformity occurs in no more than 1% of cases.

Lowering the fibular head implies a 1–2 cm leg lengthening, which significantly strengthens the cosmetic effect.
Limb lengthening is based on Ilizarov's discovery — biological tissues respond to stretching with regeneration. This is achieved by increasing the distance between the rings of the apparatus, which increases the distance between the bone fragments and stretches the tissues.
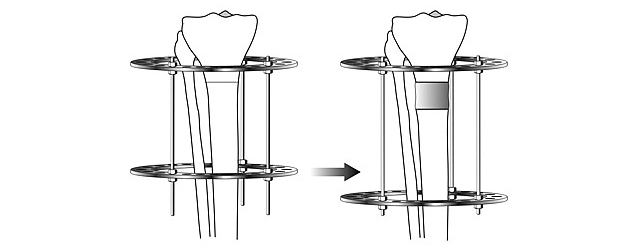

Modest lengthening (2–4 cm) for proportion optimisation significantly improves the aesthetic effect of leg-curvature correction, completely changes a person's self-image, and often their lifestyle.
The average period from surgery to apparatus removal is 3 months. For lower-leg lengthening, about 1 month per centimetre of lengthening should be added. This period assumes a gradual increase of load and activity during fixation, and the ability to fully load the legs and walk freely without restrictions immediately after the apparatus is removed.
There are the following ways to shorten the treatment:
Alternative correction methods (without the Ilizarov apparatus):
Rehabilitation is recovery after temporary functional limitations. After surgery, the restoration of motor activity must be gradual and strictly in accordance with the doctor's recommendations.
Gradual expansion of the activity regime is facilitated by modern support and mobility aids.



Clinical cases of varus knee deformity (O-legs) correction — preoperative and postoperative results performed by specialist Dr. Artemiev Alexander.
Contact us to schedule an appointment and for additional information. Our team is ready to answer all your questions.
Outpatient services, therapies and home visits are available during regular working hours.